-
 The rich enjoy life in eco-tourism properties while the land owners languish in poverty
The rich enjoy life in eco-tourism properties while the land owners languish in poverty
-
 IDC’s refusal to issue commitment letter threats to collapse a relish and sauce company
IDC’s refusal to issue commitment letter threats to collapse a relish and sauce company
-
 Anxious Easter moments as fuel price increase
Anxious Easter moments as fuel price increase
-
 Top five ANC positions in Limpopo and Mpumalanga uncontested
Top five ANC positions in Limpopo and Mpumalanga uncontested
-
 Service delivery failures in municipalities chase away investors - Ramaphosa
Service delivery failures in municipalities chase away investors - Ramaphosa
-
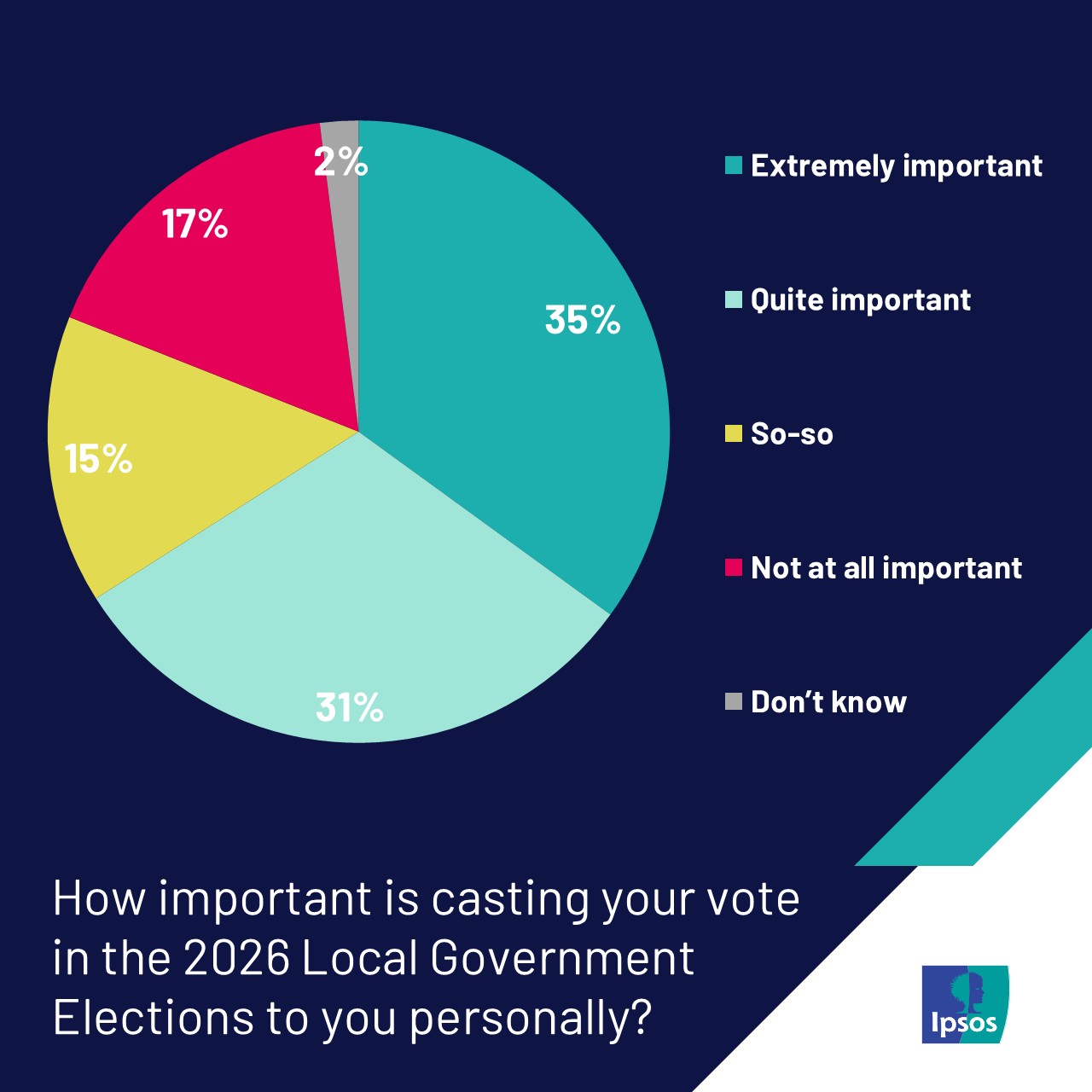 Coalition governance gaining acceptance ahead of municipal elections – Ipsos study
Coalition governance gaining acceptance ahead of municipal elections – Ipsos study
-
 Food production’s unintended climate change contribution
Food production’s unintended climate change contribution
-
 Inside a surgeon’s most defining moment of separating conjoined twins
Inside a surgeon’s most defining moment of separating conjoined twins
-
 IDC roasted for being ‘anti-black’
IDC roasted for being ‘anti-black’
-
 Call for investors and labour to be active in fighting corporate crime
Call for investors and labour to be active in fighting corporate crime
Sin taxes can save overburdened health systems in Africa
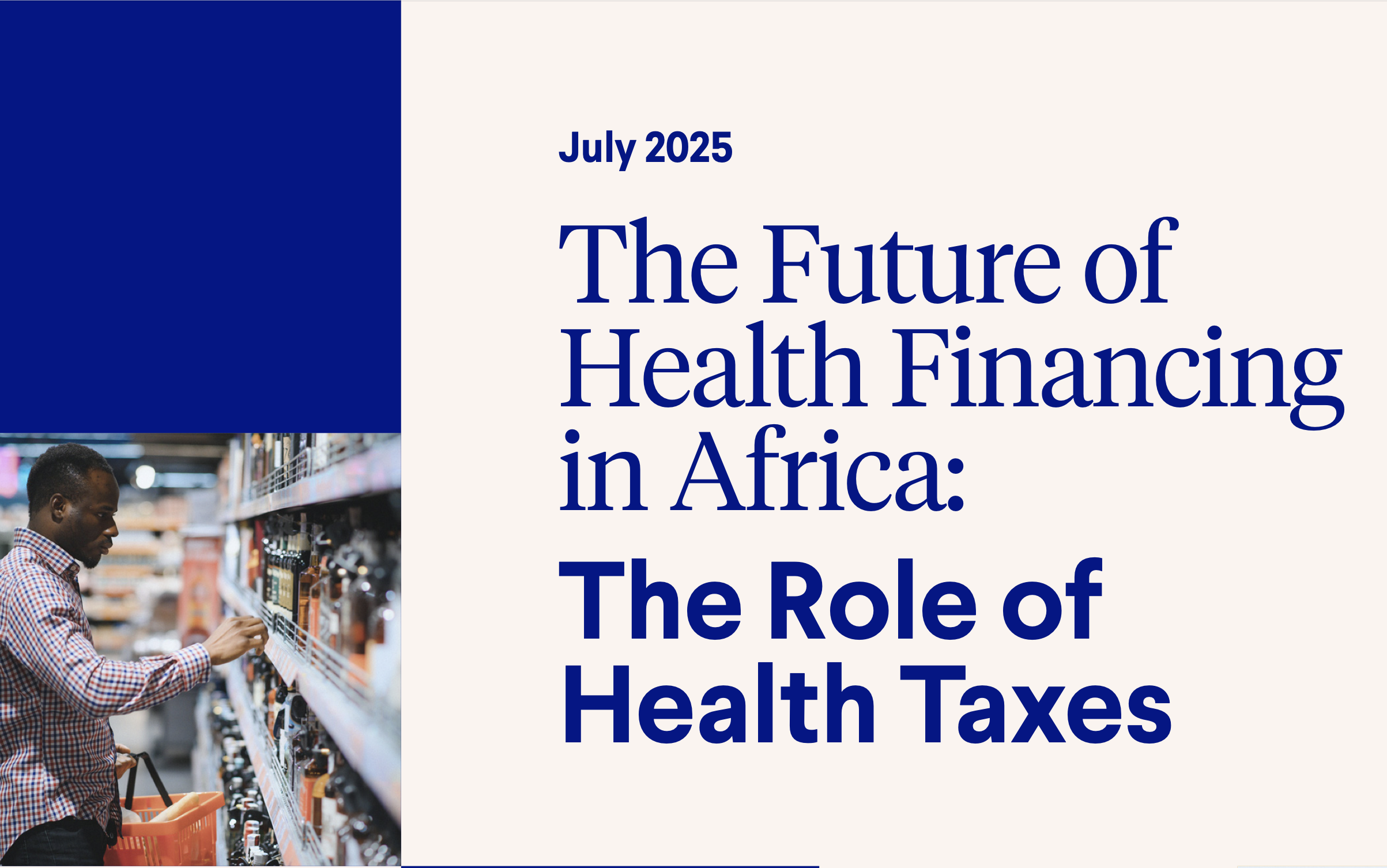
A new report by the University of the Western Cape (UWC) indicates that African countries are not leveraging on maximally taxing tobacco, alcohol and sugary drinks consumption.
Source: Supplied
Sizwe sama Yende
Africa’s public health crisis could be resolved by strengthening taxation measures on harmful products like tobacco, alcohol, and sugary drinks.
Most countries in the continent are facing a dual burden of rising noncommunicable and infectious diseases yet they are not leveraging on health taxes – excise duties on harmful products.
“As Africa confronts a mounting public health crisis, a simple yet powerful solution is being left on the table: health taxes,” according to a new report - The Future of Health Financing in Africa: The role of Health Taxes – published by Vital Strategies, the Research Unit on the Economics of Excisable Products (REEP) at the University of Cape Town’s (UCT), a research group based at Johns Hopkins University in the US.
The report indicates that health taxes could go a long way in curbing consumption of the harmful products, boosting domestic revenues and reduce reliance on the shrinking donor aid, and protecting overburdened health systems.
However, most countries were not implementing taxes to squeeze out the most revenues they could from the three biggest causes on noncommunicable diseases – tobacco, alcohol and sugary drinks.
In relation to tobacco, the median tax component of the price of tobacco products is about 41%, well below the minimum 75% that the World Health Organisation (WHO) recommends.
It is only Mauritius that has reached its maximum tax share on tobacco products – indicating that most African countries have not implemented tobacco taxes at levels sufficient to reduce consumption and increase revenues.
WHO estimates that 60 million tobacco users in the African region are over 15 years old. Tobacco use is high among adolescents – 13 to 15 years, including three million girls.
Over 200 000 deaths in Africa in each year are attributable to tobacco use. The health burden attributable to alcohol is driven by infectious diseases such as TB and HIV-Aids, injuries (road, falls, interpersonal violence) and noncommunicable diseases (liver and cardiovascular disease, cancer).
“Most African countries impose excise taxes on alcoholic beverages; however, the rates and structures are often insufficient to reduce consumption and associated harms effectively,” the report says.
Approximately 80% of countries in Africa have implemented taxes on sugary beverages. The WHO reports that 23% of countries with excise taxes on alcohol apply regular inflation adjustments.
The reports says that adoption of health taxes is often slowed down by industry influence and interference in policymaking, including exaggeration and scaremongering about job losses and illicit trade.
“These arguments rarely hold up to scrutiny: Overall employment effects are generally neutral or positive and illicit trade does not increase when enforcement is robust.”
To reduce sugary drinks consumption, says the report, taxation should be accompanied by a comprehensive approach that include: restrictions on marketing, particularly to children; limits on government procurement in settings like school; and strategic campaigns to shift consumer norms.
“Health taxes are not just a fiscal tool. They are powerful public health tools, and they save lives by curbing harmful consumption, reducing future health system costs, and providing sustainable domestic revenue to ease dependence on shrinking aid flows,” said REEP’s director, Professor Corné van Walbeek.
“These products – tobacco, alcohol and sugary drinks – are not only contributing heavily to preventable deaths, they are placing unsustainable pressure on health systems. Failing to tax them appropriately costs us lives and valuable resources,” Walbeek added.
The report argues that, beyond the public health argument, the economic rationale for health taxes is compelling. As development assistance declines and domestic budgets tighten, well-designed health taxes offer a stable and predictable revenue stream. When adjusted for inflation and income growth, and paired with robust enforcement, health taxes can support governments to build more resilient health systems, especially in the face of growing urbanisation and changing population demographics.
Examples from across the continent demonstrate the feasibility and impact of such taxes. For example, in South Africa, the introduction of the Health Promotion Levy has been associated with a measurable decline in sugar consumption. In Kenya, higher tobacco and alcohol taxes have helped curb use, particularly among young people. Botswana and Ghana are exploring further adjustments to improve the effectiveness of their health tax regimes.
“The notion that health taxes are regressive is misleading,” said Van Walbeek. “Over time, these taxes are progressive because they reduce disease and financial hardship among the most vulnerable populations. The health benefits from reduced consumption of unhealthy products are greatest for low-income communities, because they are the most responsive to a tax-induced increase in the prices of these products.”